Scientific Data Surah 103 · Ayah 1
The importance of time
The importance of time
Abstract
Endovascular treatment (EVT) of severe acute ischemic stroke (AIS) determined by large vessel occlusion (LVO) is effective and safe. Debate still goes on especially about time importance and utilization of advanced penumbra imaging at the expense of loosing valuable minutes.
⦁ Methods
We did a meta-analysis focused on time of randomized clinical trials (RCTs) that started to use methodically the new-tech stent retrievers. The chosen time interval was onset-groin time (from last seen well to sheath insertion in the cathlab). Primary outcome was good functional outcome (mRS of 0–2) at 90 days, and secondary outcomes were mortality at 90 days and symptomatic intra-cerebral hemorrhage (sICH). Furthermore, we did a sub-analysis of the EVT patients to find a correlation between faster times and outcomes. We did the same sub-analysis including also single-arm registries that used modern stent retrievers.
⦁ Results
Totally data from 1287 patients (5 RCTs) were analyzed, whose 634 EVT patients were divided into two groups based on time (faster/slower than 240 min). Furthermore 1501 EVT-treated patients (9 studies) were divided into two pre-specified groups (fast/slow) and analyzed. In both meta-analysis and sub-analysis, the fast group had better functional outcome at 90 days [log OR = −2.07, 95% CI (−3.00, −1.14)] and less deaths [log OR = −0.56, 95% CI (−3.66, −2.55)], demonstrating that onset-groin time has a strong impact even on mortality. On the other hand, sICH resulted to be more frequent in the slow group [log OR = 0.18, 95% CI (−1.36, −1.71)] emphasizing how delays could even worsen AIS.
⦁ Conclusions
This meta-analysis supports the “Time is brain” strategy in treatment of acute ischemic stroke. In general, fast endovascular treatment (groin puncture within 4 h) significantly improves patients’ outcomes. Healthcare systems should develop maximal effort to shorten pre-hospital and in-hospital delays in acute stroke patients. The earlier the patient is presenting, the more important is the fast track, offering chance for full neurologic recovery.
Keywords
⦁ Acute ischemic stroke ,Endovascular therapy, Thrombectomy ,Catheter-based therapy
Introduction
Ischemic stroke is one of the most important causes of death and severe functional disability around the world nowadays, with a very high human price and a strong impact on healthcare systems. Intra-venous rtPA (iv rtPA) initiated up to 4.5 h from symptom onset is indicated for acute ischemic stroke (AIS) based on the 2013 American Heart Association (AHA) Guidelines [1]. The latest 2015 update from AHA [2] introduced 1A indication for endovascular therapy(EVT) after five recent randomized controlled trials [3], [4], [5], [6], [7], [8] (RCT) strongly supported the use of EVT in specifically selected patients, in particular those with evidence of large clots in the distal internal carotid artery (ICA) or in the middle cerebral artery(segment M1 or M2) and with a severe clinical presentation (high NIHSS). Before these successful RCTs, there were three neutral trials during 2013 [9], [10], [11] that were not able to demonstrate benefit from EVT due to suboptimal patient selection and old technology (modern thrombectomy retrievers used only in minority of patients). Going through the recent RCTs, we can point out some differences in methodology and inclusion criteria that could be underestimated or misinterpreted. The net benefit in terms of good functional outcome for EVT in comparison with the control iv rtPA-alone groups on the eligible patients is now confirmed by recent meta-analysis and review articles [12], [13], [14], [15], [16] and the importance of time to revascularization is highlighted by several studies about iv rtPA [17] or EVT [18], [19], [20]. We aimed to investigate the influence of time delays on the major outcomes of AIS treated by EVT in the current stent retrievers’ era.
Methods ⦁ Data sources
We searched PubMed, Cochrane CENTRAL, Web of Science, and the National Institutes of Health Clinical Trials from 1 January 1995 (year of publication of the NINDS rtPA Stroketrial) through 30 October 2015, for English language, peer-reviewed publications. The following Medical Subject Heading terms and/or keywords were used for database searches: ‘acute ischemic stroke’, ‘intra-arterial therapy’, ‘endovascular treatment’, ‘endovascular therapy’, ‘thrombectomy’, and ‘catheter-based treatment’. Related reviews, clinical trial databases and the reference lists of all retrieved articles were also searched manually for relevant studies. Any disagreements were resolved by discussion.
⦁ Study selection and eligibility criteria
We included trials with at least 12 weeks of follow-up, both double-blind and open-label trialdesigns were eligible for inclusion. We followed the PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) statement for reporting systematic reviews and meta-analyses of RCTs for our protocol [21].
We decided to analyze manuscripts that started to use mechanical thrombectomy with modern stent-retrievers, excluding the neutral 2013 RCTs for their methodology limits already highlighted in other papers [22], [23], in particular for their limited use of these last generation devices.
⦁ Choice of times and outcomes
We decided to compare the time from the stroke onset (or last seen well) to the sheath insertion in the cathlab (onset-groin time) because it is the most relevant time interval across the studies and the only one always present in all the EVT arms.
The primary specified outcome was the proportion of patients with a good functional outcome defined with the modified Rankin Scale (mRS of 0–2) at 90 days from stroke onset. Secondary outcomes included mortality at 90 days and symptomatic intra-cerebral hemorrhage (sICH). Asymptomatic ICH was defined in different ways across the RCTs so it was excluded from the analysis.
⦁ Statistical analysis
Key statistical analysis was conducted by an external independent statistician (B.P.).
To compare the results in different studies the forest chart from metaphor package of program R was used (http://cran.r-project.org/). The problem for quantitative data was that for the same variables were used different descriptions in the different studies: mean and SD, or median and quartiles, or median and minimum and maximum. To solve this problem, we supposed normal distribution and estimated mean as median and we estimated SD from normal distribution with appropriate quartiles, respect to maximum and minimum.
The estimated median onset-groin time was 229.9 min for the EVT arm patients so we decided to dichotomize them in two pre-specified groups (fast/slow): faster or slower than 4 h (240 min) to see the impact of time on outcomes.
For representation of the results we use forest plot (for all, iv rtPA/EVT arms, fast/slow groups) of logarithmic odds ratio (log OR) and their 95% confidence interval (95% CI). To compare the impact of iv rtPA/EVT arms or fast/slow groups we used bootstrappingANOVA model with nuisance categorical parameter [24]. For the qualitative variables we used the forest charts and the Mantel–Haenszel test with nuisance categorical parameter [25].
Moreover, we made crude odds ratio (OR) to directly compare fast/slow groups inside the EVT arms, using analysis of contingency tables (chi-square or Fisher's test) to calculate the association between qualitative variables thus correlating outcomes with the two pre-specified groups [25]. We considered significance level of 5% (p < 0.05).
Results
⦁ Included studies
Totally 3741 articles were found in the databases and only 27 met eligibility criteria for full text evaluation. Of these, we did a meta-analysis of the five recent trials starting from the end 2014 (MR CLEAN) to have a comparison between time and the different outcomes in all these successful RCTs; we did also a sub-analysis to correlate time and outcomes only in the EVT treated patients (fast/slow groups).
Moreover, we did a sub-analysis (crude OR) including also single arm registries [26], [27], [28], [29] to make a direct comparison between time and the different outcomes only between EVT arms of these nine studies.
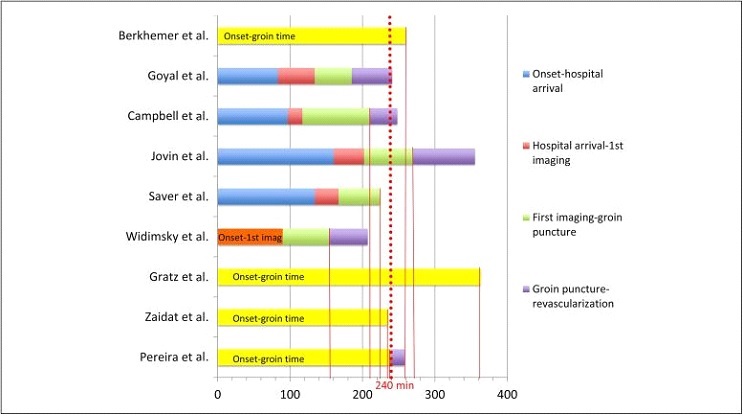
Study characteristics are shown in Table 1 and the different time intervals of the included studies in Fig. 1.
⦁ Table 1

CTA, CT angiography; DSA, digital subtraction angiography; EVT, endovascular therapy; iv rtPA, intra-venous plasminogen activator; MRA, MR angiography; mRS ≤2, good functional outcome; NA, not assessed; NIHSS, National Institutes of Health Stroke Scale; RCT, randomized controlled trial; sICH, symptomatic intra-cerebral hemorrhage; TICI, modified Thrombolysis in Cerebral Infarction.
Symptomatic intracranial hemorrhage was defined as parenchymal hemorrhage type 2 on follow-up imaging and neurologic deterioration of at least four points on the NIHSS, according to the Safe Implementation of Thrombolysis in Stroke – Monitoring Study (SITS-MOST) criteria, or any symptomatic intracranial hemorrhage and neurologic worsening of at least four points on the NIHSS, according to the second European–Australasian Acute Stroke Study (ECASS II) criteria.
⦁ RCT meta-analysis and sub-analysis
A total of 1287 patients were included from the 5 RCTs, 634 for EVT arms and 653 for control arms (mostly iv rtPA). Dividing the EVT arms in two groups based on time, we have a total of 298 patients in the fast group (mean onset-groin time 207.64 min) and 336 in the slow one (mean onset-groin time 263.83 min).
There were no differences between the two groups in mean age (fast group 68.01 versus slow group 65.74, [CI for difference (−4.25, 8.78), p = 0.248]), ASPECT score (9 versus 8, [CI for difference (−1.78, 3.78), p = 0.24]) and NIHSS (16.67 versus 17.00, [CI for difference (−4.31, 3.64), p = 0.434]).
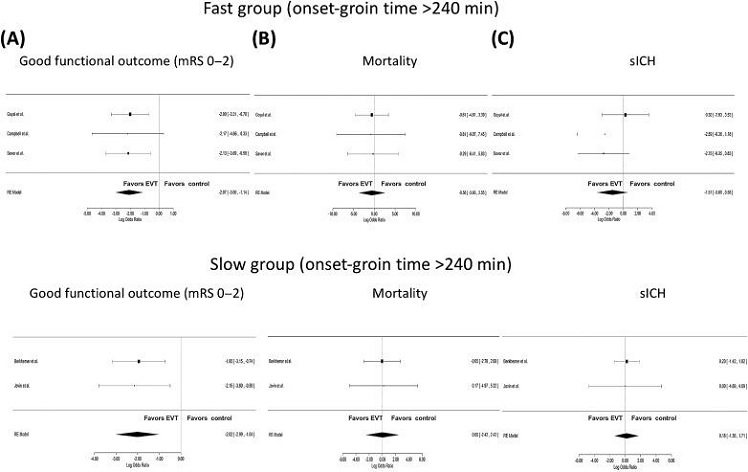
The pooled log odds ratio for primary and secondary outcomes is shown in Fig. 2 and the crude OR with p-value is shown in Table 2.
⦁
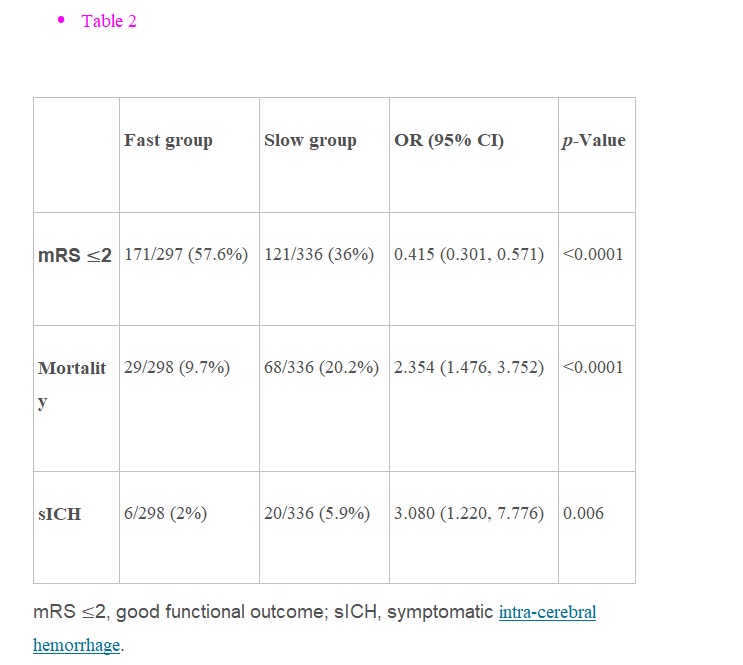
Good functional outcome was achieved from 46% of patients treated with EVT against 26% of controls with significant difference [log OR = −2.05, 95% CI (−2.72, −1.37)]. The fast group has a higher difference of log OR for good functional outcome than the slow (−2.07 versus −2.02). Comparing fast/slow groups 171 patients (57.6%) had good functional outcome versus 121 (36%) with a statistically significant difference [OR = 0.415 (0.301, 0.571), p < 0.001].
Deaths were 14.5% in the EVT arms versus 17.3% in the controls, not significantly different [log OR = −0.21, 95% CI (−2.12, 1.70)].
Looking into crude OR, mortality results significantly correlated with time in favor of the fast group with 29 deaths versus 68 [OR = 2.354 (1.476, 3.752), p < 0.001].sICHs have a trend in favor of the EVT arm [log OR = −0.48, 95% CI (−1.78, 0.81)] and looking to the fast group, this trend becomes even bigger (−1.51 versus 0.18 for the slow group). Based on the crude OR, sICHs were significantly lower in the fast group [OR = 3.080 (1.220, 7.776), p = 0.006].
⦁ EVT studies sub-analysis
A total of 1501 patients from 9 studies were divided in the two pre-specified groups: 811 patients from six studies in the fast group (mean onset-groin time <240 min) and 690 from three studies in the slow group (>240 min).
The crude OR with p-value is shown in Table 3.
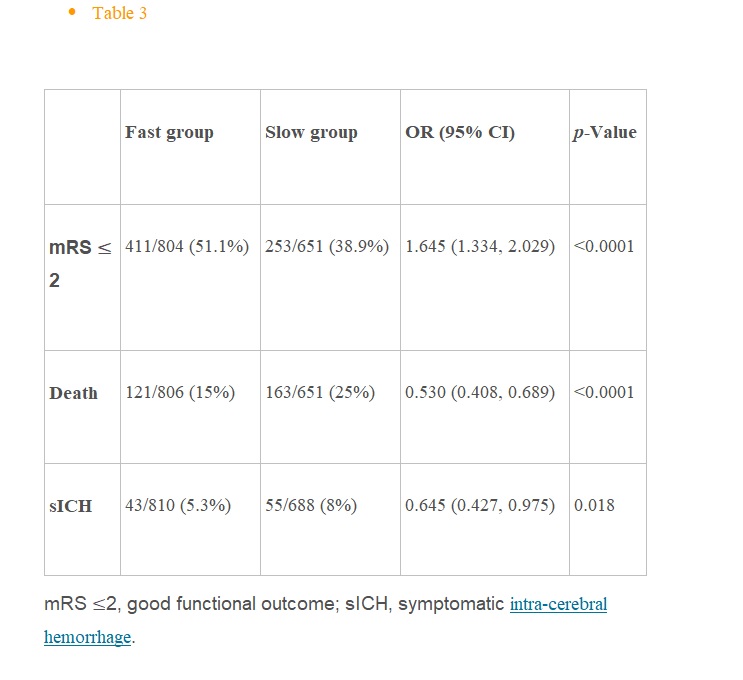
For the fast group 411 patients (51.1%) had good functional outcome against 253 for the slow group (38.9%) with a statistically significant difference [OR = 1.645 (1.334, 2.029), p < 0.001]. Looking to mortality, deaths were considerably lower in the fast group than in the slow [121 patients (15%) versus 163 (25%): OR = 0.530 (0.408, 0.689), p < 0.001]. Also sICHs were less for the fasters than for the slowers with statistically significant difference [OR= 0.645(0.427, 0.975), p = 0.036].
Discussion
In this study we highlighted the importance of time delays in managing the hyperacute phase of ischemic stroke and our results confirmed that all the outcomes are improved when the onset-groin time is shortened. In both meta-analysis and sub-analysis, the fast group has better functional outcome at 90 days and less deaths, demonstrating that onset-groin time has a strong impact even on mortality. On the other hand, it is impressive how sICH results to be more frequent in the slow group emphasizing how time could play a role in the development of the major complication of AIS.
From our interventional cardiology background, time runs faster for brain than for muscle in the heart: it was estimated that each minute 1.9 million neurons, 14 billion synapses and 12 km of myelinated fibers are destroyed [30].
From a recent meta-analysis [20] it seems that for every thousand patients treated, every 15-min acceleration is associated with a 34 more patients having reduced final disability by one or more levels on the mRS and that for every 5-min delay in endovascular reperfusion, 1 out of every 100 patients treated has a worse disability outcome.
We want to focus on the logistic organization of the out-of-hospital and in-hospital stroke network, trying to find some critical points that could improve the onset-reperfusion time.
We strongly believe that the stroke care community needs the more simplified clinical-diagnostic algorithm to discriminate the acute stroke patients that could benefit from EVT, especially for those with onset-groin time <4 h (early comers).
As for the STEMI guidelines development during the last 20 years, in which we assisted how ECG played a paramount role in discriminating patients that need a primary PCI versus the others that can wait for a belated interventional approach, we need a “black&white” criterion able to direct to the cathlab this group of patients that could benefit from prompt EVT.
The pivotal role of CT angiography is now clear and it is considered mandatory to define large vessel occlusion (LVO) strokes while there is still big debate on the use of additional advanced penumbra imaging (API) to assess perfusion or collateral circulation, over the basic CT to exclude ICH and define the infarct area. In hyperacute stroke management, there is the need of a super-fast imaging protocol to minimize the onset-1st imaging-groin time intervals, avoiding any useless loss of time.
Even if the trials that used API had the highest proportion of patients with mRS 0–2 at 90 days, the knowledge of the number of patients who were excluded by various imaging approaches is incomplete. EXTEND-IA is the only trial that reported reasons for exclusion based on screening log data: of patients treated with rtPA, 495 of 1044 (47%) were excluded because of an absence of evidence for LVO on CT angiography and only a little proportion of patients (4% overall) were excluded by perfusion imaging criteria [31].
A group of studies [32], [33], [34] support the idea that time is less important than demonstrating salvageable brain tissue with a perfusion–diffusion mismatch: Lansberg et al. [32] state that “because time is an imprecise surrogate for the presence of salvageable brain tissue, it is also an imperfect criterion for selecting patients who are likely to benefit from reperfusion”. This opinion could keep the community in the wrong direction, we cannot focus our attention on this percentage of patients that for different reasons has a stable penumbra as time goes on (different stroke pathophysiology, very good collateral circulation) but we all need to accelerate the triage system to allow that the number of early-comers will grow and all the initiatives to shorten the intra-hospital logistics, comprising the fastest imaging protocol to keep in the cathlab patients with LVO.
For this purpose, it could be useful to develop a score system to identify severe strokes (NIHHS >15) with LVO at the time of stroke onset, especially in the out-of-hospital setting [35]. Moreover, there are some studies that tested the usage of ambulances working as mobile stroke unit with the possibility to perform 1st-imaging and start iv rtPA, to direct properly AIS patients to Primary Stroke Centers and to further shorten the onset-groin time thus annulling the door-1st imaging time [36], [37].
Coming back to both DEFUSE-2 [32] and Prabhakaran's multi-center registry [33], onset-groin times were longer than 4 h so it is not possible to have a direct comparison between those who had API with a group of real early-comers that could benefit of a fast-track approach. Furthermore, API techniques are paramount for evaluation of the late-arrivals, intended as patients with onset-groin time longer than 6 h, and it is reasonable to extend the EVT window to 12–24 h for this group of patients with still a high amount of salvageable tissue demonstrated by API, looking forward for the results of the ongoing DAWN and POSITIVE trials.
But the major purpose of AIS community should be to speed up all the healthcare systems to avoid these delays to still happen; there are some centers that experimented successfully a collaborative cardio-neurologic cooperation [29], exploiting a tested and effective system for out-of-hospital care as the STEMI networks and a 24/7 emergency service (maybe with the double alert system), bypassing emergency room and intensive care unit, thus going directly to CT suite and after to the cathlab or better with a fast-track single-stop approach [38], without useless in-hospital transfers [39].
The helping hand of the interventional cardiologist is now offered, the stroke community should be interested in shaking it.
Conclusion
This meta-analysis supports the “Time is brain” strategy in treatment of acute ischemic stroke. In general, fast endovascular treatment (groin puncture within <4 h) significantly improves patients’ outcomes. Healthcare systems should develop maximal effort to shorten pre-hospital and in-hospital delays in acute stroke patients. The earlier the patient is presenting, the more important fast track is offering chance for full neurologic recovery.
Conflict of interest
No conflict of interest.
Ethical statement
I declare, on behalf of all authors, that the research was conducted according to Declaration of Helsinki.
Informed consent
I declare that informed consent requirements do not apply to this manuscript.Funding body None.
SOURCE:
Reference Link